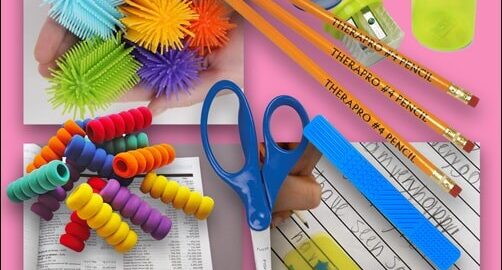
Therapro’s Everyday Classroom Kit is the newest kit to hit our shelves. This kit was created with the thought of students returning to classrooms under new pandemic guidelines. Therapro’s Everyday Classroom Kit includes all the essentials for day to day classroom use and is intended for a single user. In this way every student has the essential items they need for classroom participation while minimizing the sharing of these commonly used classroom essentials! Included in each kit are:
- 1 Standard Size Pencil With #4 Jumbo Lead
- 1 Swirl Foam Grip
- 1 Spike Tactile Pencil Topper
- 1 Fiskars Blunt-tip Kids 5″ Scissors
- 1 Sensory Bookmark
- 1 Two Hole Pencil Sharpener
- 1 Star Spacer
- 1 Reading Guide Strip
Set your pencil up right! Included in each kit is a Standard Size Pencil With #4 Jumbo Lead and just the right accessories, a Swirl Foam Grip and a Spike Tactile Pencil Topper! These are just the right pencil accessories for comfort and increased focus during writing tasks. The swirl foam grip can be used by every student, it is not meant to correct grip instead it is simply for comfort. The Spike Tactile Pencil Topper is a great accessory for every student; this small fidget is a great way to improve attention and focus!
Improve handwriting legibility! Included in each kit is the The Star Spacer; the Star Spacer is a clever handwriting tool made of see-through plastic which acts as a guide to help the child understand spacing, sizing, and alignment of letters and words to promote more legible handwriting. The blue star printed on the spacer is a great reminder for both letter size and space between words. Here’s a bonus tip, turn it vertically to help line up columns of numbers during math work!
Increase attention and focus! Included in each kit is the Reading Guide Strip. The Reading Guide Strip is a great tool to help all students attend to and focus during reading tasks. The Reading Guide Strips helps students track print through it’s transparent, tinted windows; a great way to improve attention when reading!
To round out this kit we included three “must have” classroom essentials; Fiskars Blunt-tip Kids 5″ Scissors, The Sensory Bookmark, and a Transparent Two Hole Pencil Sharpener! Scissors, bookmarks, and pencil sharpeners are frequently used multiple times through the course of a typical school day; by providing each student one of their own you can decrease cross contamination! The Sensory Bookmark doubles as a fidget; users can run their fingertips across four different textured sections!